“Precisely targeted radiation therapy can eradicate all evidence of disease in selected patients with cancer that has spread to only a few sites, suggests the first published report from an ongoing clinical trial. … Six of the 29 [21%] initial patients had lasting tumor control, with no detectable evidence of disease 15 months after treatment. Many patients had a complete response in at least one tumor. Thirty-one of the 56 treated tumors (55%) completely disappeared. Two tumors (4%) had a partial response, defined as reduction in tumor volume of more than 30 percent. Only three of the 56 tumors progressed (5%), growing in size by 20 percent or more during the treatment phase … Crucial to this approach is careful patient selection, distinguishing between patients who have a treatable number of tumors and those who have widespread metastasis, including multiple tumors too small to detect. Currently, there are no known genetic “signatures” to differentiate between widespread cancer versus oligometastasis, the authors point out.”

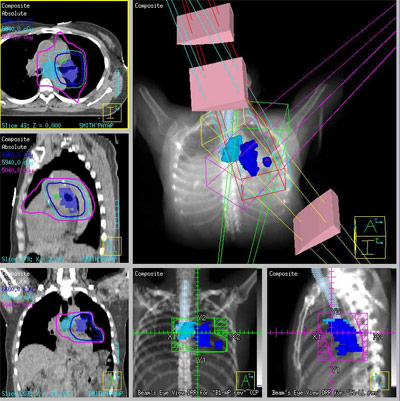
Image-Guided Radiation Therapy (IGRT) Used To Treat "Oligometastasis"
“Precisely targeted radiation therapy can eradicate all evidence of disease in selected patients with cancer that has spread to only a few sites, suggests the first published report from an ongoing clinical trial.
In the August 15, 2008, issue of Clinical Cancer Research, (published online August 12) researchers from the University of Chicago Medical Center report that targeted radiation therapy had completely controlled all signs of cancer in 21 percent of patients who had five or fewer sites of metastatic disease.
‘This was proof of principle in patients who had failed the standard therapies and had few, if any, remaining options,’ said the study’s senior author, Ralph Weichselbaum, MD, professor and chairman of radiation and cellular oncology at the University of Chicago Medical Center. “We had encouraging results, including several long-term survivors, in patients with stage-IV cancers that had spread to distant sites.’
In 1994, Weichselbaum and colleague Samuel Hellman proposed that there was an intermediate state between cancer that had not spread at all and cancer that had spread extensively. They named this phenomenon “oligometastases,” meaning cancer that had spread to a few distant sites.
In some cases, surgeons have successfully treated such limited cancer spread, producing long-term survival by removing the primary cancer and one or two distant tumors, off-shoots of the original cancer–usually in the lung or liver. However, some patients are not fit for surgery or have cancer that is inoperable.
Recent improvements in tumor detection and precise image-guided radiation therapy, however, have made simultaneous treatment of multiple tumor sites with radiation feasible. So in 2004, Weichselbaum organized a clinical trial to test the ability of local radiation therapy to control a limited number of related tumors which colleague Joseph Salama, MD, assistant professor of radiation oncology at the University of Chicago has directed since 2005.
Patients with stage-IV cancer with one to five distant metastases and no tumors bigger than 10 centimeters (about four inches) in diameter were eligible to participate in the study either before or after chemotherapy treatment.
Each patient received three doses, separated by at least two days, of precisely targeted radiation therapy focused on each metastatic tumor. Treatment was usually completed within one week. The first patients in the study received lower doses. As few side effects were seen, radiation doses were gradually increased in subsequent groups of patients.
‘Previous studies determined the maximal radiotherapy doses for single organs,’ said Salama, lead author of the study, ‘but this technique has not been tested for simultaneous use on multiple organs. So we designed a dose-escalation trial to determine the optimal dose, starting with fairly low levels and increasing the dose in later groups of patients.’
From November 2004 through February 2008, 29 patients, with a total of 56 cancerous lesions, enrolled in the trial. Of the 29 patients, 24 had progressed after at least one round of systemic chemotherapy. For the other five, there was no promising choice of therapy.
Six of the 29 initial patients had lasting tumor control, with no detectable evidence of disease 15 months after treatment.
Many patients had a complete response in at least one tumor. Thirty-one of the 56 treated tumors (55%) completely disappeared. Two tumors (4%) had a partial response, defined as reduction in tumor volume of more than 30 percent. Only three of the 56 tumors progressed (5%), growing in size by 20 percent or more during the treatment phase.
Tumor control improved as the radiation dose increased. Thirty-nine percent of the 31 tumors treated with 24 gray of radiation met the criteria for tumor control–a complete or partial response. That increased to 79 percent for the 19 tumors treated with 30 gray, and to 83 percent for the six tumors treated with 36 gray.
‘This suggests that the initial doses were too low,’ said Salama. ‘We have seen improved response rates with higher radiation doses without an increase in side effects yet.’
Typical treatment doses for a patient with breast cancer, for example, are in the range of 50 to 60 gray, spread over 20-30 sessions. The trend however, is toward delivering higher doses in fewer sessions.
Patients tolerated the treatment, the authors write, with ‘limited difficulty.’ All had some fatigue but few had serious side effects. The most severe included one patient being treated for abdominal tumors who developed vomiting that required hospitalization. One lung cancer patient developed a severe cough. One patient had gastrointenstinal [sic] bleeding three months after treatment that required blood transfusion and laser treatment.
Crucial to this approach is careful patient selection, distinguishing between patients who have a treatable number of tumors and those who have widespread metastasis, including multiple tumors too small to detect. Currently, there are no known genetic “signatures” to differentiate between widespread cancer versus oligometastasis, the authors point out. This is one area of active research. Only five of the 29 patients treated so far, however, had tumor progression in more than five sites.
The technique could also be applied after chemotherapy, the authors suggest, in cases where the drugs had eliminated most the smaller cancer, leaving only a few larger tumors behind.
The trial is still underway. ‘We now have about 50 patients,’ said Weichselbaum, ‘and several of them remain disease-free, one of them three years after treatment.’
The Ludwig Center for Metastasis Research and the University of Chicago Cancer Research Center funded this study. Additional authors include Steven Chmura, Neil Mehta, Kamil Yenice, Walter Stadler, Everett Vokes, Daniel Haraf and Samuel Hellman, of the University of Chicago Medical Center.”
Quoted Source: Targeted Radiation Therapy Can Control Limited Cancer Spread, Press Release, The University of Chicago Medical Center, August 15, 2008 (summarizing the findings of An initial report of a radiation dose-escalation trial in patients with one to five sites of metastatic disease; Salama JK et. al., Clin Cancer Res. 2008 Aug 15;14(16):5255-9. (” … RESULTS: Twenty-nine patients with 56 metastatic lesions were enrolled from November 2004 to March 2007, with a median follow-up of 14.9 months. Two patients experienced acute (radiation pneumonitis and nausea) and one experienced chronic (gastrointestinal hemorrhage) grade >/=3 toxicity. Fifty-nine percent of patients responded to protocol therapy. Twenty-one percent of patients have not progressed following protocol treatment. Fifty-seven percent of treated lesions have not progressed at last follow-up. Progression was amenable to further local therapy in 48% of patients. CONCLUSIONS: Patients with low-volume metastatic cancer can be identified, safely treated, and may benefit from radiotherapy.”))
Additional Information: