This year, approximately 565,650 Americans are expected to die of cancer — that’s more than 1,500 people a day. … Ovarian cancer causes more deaths than any other cancer of the female reproductive system. … In an unprecedented television event, NBC, ABC, and CBS will simultaneously devote 1 hour of commercial-free prime time to raise funds for the fight against cancer under an initiative called “Standup2cancer.”

What Do You Stand For?
- This year, approximately 565,650 Americans are expected to die of cancer — that’s more than 1,500 people a day.
- Cancer is the second most common cause of death in the US, exceeded only by heart disease. In the US, cancer accounts for 1 of every 4 deaths.
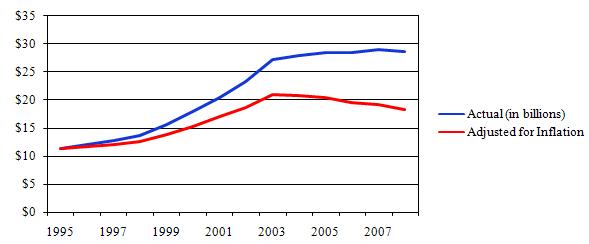
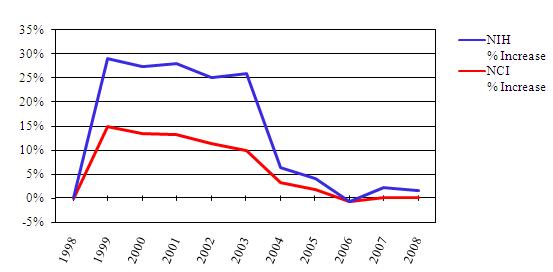
- The budgets for the National Institutes of Health (NIH) and the National Cancer Institute (NCI) have been flat for 5 years. Adjusted for inflation, the NIH budget has fallen 13 percent since 2003, and the NCI budget has fallen 12 percent since 2004.
- The NIH estimate overall costs of cancer in 2007 at $219.2 billion:
- $89.0 billion for direct medical costs;
- $18.2 billion for lost productivity due to illness; and
- $112.0 billion for lost productivity due to premature death.
- Ovarian Cancer can afflict adolescent, young adult, and mature women, although the risk of disease increases with age and peaks in the late 70s. Pregnancy and the long-term use of oral contraceptives reduce the risk of developing ovarian cancer.
- Women who have had breast cancer, or who have a family history of breast cancer or ovarian cancer may have increased risk. Inherited mutations in BRCA1 or BRCA2 genes increase risk. Another genetic syndrome, hereditary nonpolyposis colon cancer, has also been associated with endometrial and ovarian cancer.
- Ovarian cancer incidence rates are highest in Western industrialized countries.
- Ovarian cancer accounts for about 3% of all cancers among women and ranks #2 among gynecologic cancers.
- An estimated 21,650 new ovarian cancer cases are expected in the U.S. in 2008.
- An estimated 15,520 ovarian cancer deaths are expected in 2008.
- Ovarian cancer causes more deaths than any other cancer of the female reproductive system.
- Ovarian cancer is not a “silent” disease; it is a “subtle” disease. Recent studies indicate that some women may experience persistent, nonspecific symptoms, such as (i) bloating, (ii) pelvic or abdominal pain, (iii) difficulty eating or feeling full quickly, or (iv) urinary urgency or frequency. Women who experience such symptoms daily for more than a few weeks should seek prompt medical evaluation. (To learn more about the warning signs and symptoms of ovarian cancer, CLICK HERE).
- There is no reliable screening test for the detection of early stage ovarian cancer. Pelvic examination only occasionally detects ovarian cancer, generally when the disease is advanced. However, the combination of a thorough pelvic exam, transvaginal ultrasound, and a blood test for the tumor marker CA125 may be offered to women who are at high risk of ovarian cancer and to women who have persistent, unexplained symptoms like those listed above.
- If diagnosed at the localized stage, the 5-year ovarian cancer survival rate is 92%; however, only about 19% of all cases are detected at this stage, usually fortuitously during another medical procedure.
- For women with regional and distant metastatic disease, the 5-year ovarian cancer survival rates are 71% and 30%, respectively. The 10-year relative survival rate for all stages combined is 38%.
- During 1987-2004, ovarian cancer incidence declined at a rate of 0.9% per year.
Sources: Cancer Facts & Figures 2008, American Cancer Society (Adobe Reader PDF); There Are Many Ways To Fight Cancer. Cutting Funding For Research Isn’t One of Them, by Paul Cacciatore, Libby’s H*O*P*E* post, June 10, 2008.
Tonight, over 50 of the most renowned personalities in TV, film, sports and music will come together to make history. In an unprecedented television event, NBC, ABC, and CBS will simultaneously devote 1 hour of commercial-free prime time to raise funds for the fight against cancer under an initiative called “Standup2cancer.” In May, Libby’s H*O*P*E*™ covered the opening of the Standup2cancer initiative. [May 30, 2008].
A spectacular line up of talent including Jennifer Aniston, James Taylor, Scarlett Johansson, Meryl Streep, David Cook, Christina Applegate, Lance Armstrong, Jack Black, Kirsten Dunst, Charles Barkley, America Ferrera, Halle Berry, Hilary Swank, Forrest Whitaker, Jimmy Fallon, Keanu Reeves will make personal appearances on the show. These celebrities and more will educate you, move you and entertain you. They will also be on hand to answer your calls in the celebrity phone bank.
To donate, CLICK HERE. The YouTube video below provides an explanation of how the public donations will be used.
SU2C: Where the Money Goes?
The premiere TV performance of “Just Stand Up” – the star studded charitable single in support of Stand Up To Cancer will be performed tonight by legendary recording artists Mariah Carey, Beyonce, Mary J. Blige, Rihanna, Fergie, Sheryl Crow, Miley Cyrus, Melissa Etheridge, Ashanti, Natasha Bedingfield, Keyshia Cole, Ciara, Leona Lewis, LeAnn Rimes, and Carrie Underwood.
Just Stand Up! – Standup2cancer