The expert panel discussion was divided into the two sessions listed below. Click here if you are interested in watching the webcast version of each session. A transcript of each session is also provided below.
“… Our study shows that percutaneous CT-guided radiofrequency ablation yields high proportions of sustained [complete responses] in properly selected patients with primary or secondary lung malignancies, and is associated with acceptable morbidity,’ write the authors.”
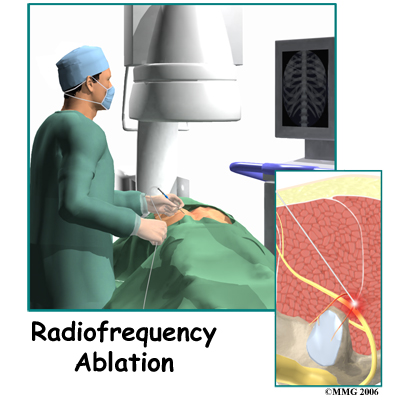
Percutaneous radiofrequency ablation is a relatively new and minimally invasive technique that has been used to treat solid tumors. In particular, it is becoming a viable option for unresectable liver malignancies. Although the use of radiofrequency ablation is at an early stage of clinical application for other types of solid tumors, recent studies have shown that it has potential in the treatment of lung, bone, and renal malignancies. The authors note that several single-institution case series have suggested that radiofrequency ablation is a feasible option for patients with unresectable or medically inoperable pulmonary tumors.
In this study, Riccardo Lencioni, MD, associate professor of radiology in the department of oncology, transplants and advanced technologies in medicine at the University of Pisa, in Italy, and colleagues designed a prospective single-group multicenter clinical trial to evaluate the feasibility, safety, and effectiveness of percutaneous computed tomography (CT)-guided radiofrequency ablation in the treatment of NSCLC. The study also included patients with metastatic disease to the lungs.
A series of 106 patients, with a total 183 lung tumors measuring 3.5 cm or smaller in diameter, were enrolled in the study. Of this group, 33 patients had been diagnosed with NSCLC, 53 had metastasis from colorectal carcinoma, and 20 patients had metastasis from other primary malignancies. All of the patients were deemed unsuitable for surgery, radiotherapy, or chemotherapy.
The primary end points were technical success, safety, and confirmed complete response of tumors. The authors defined technical success as the correct placement of the ablation device in all target tumors with completion of the planned ablation protocol. Secondary end points of the study included overall survival, cancer-specific survival, and quality of life.
Study participants underwent radiofrequency ablation in accordance with standard rules for CT-guided lung biopsy. Follow-up visits were scheduled at 1 and 3 months after the procedure, and then at 3-month intervals for up to 2 years.
A total of 137 procedures were performed, and treatment was successfully completed in 105 of 106 patients (99%). From this group, it was possible to assess the primary end point of a confirmed complete response in 85 patients (80%). The researchers noted a confirmed complete response of all targeted tumors that lasted for at least 1 year after treatment in 75 of 85 patients (88%), with incomplete ablation and evidence of local progression in at least 1 treated tumor in the remaining patients. There was no difference in tumor responses to ablation between patients with NSCLC and those with metastatic lung disease.
Overall and Cancer-Specific Survival
Patient Subgroup
Overall Survival at 1 Year
Overall Survival at 2 Years
Cancer-Specific Survival at 1 Year
Cancer-Specific Survival at 2 Years
NSCLC
70%
48%
92%
73%
Stage 1 NSCLC
n/a
75%
n/a
92%
Colorectal metastases
89%
66%
91%
68%
Metastases from other sites
92%
64%
93%
67%
Although there was no procedure-related mortality, 27 of the procedures were complicated by a large or symptomatic pneumothorax that required drainage. A second major complication was the occurrence of pleural effusion in 4 procedures, which also necessitated drainage.
‘Our study shows that percutaneous CT-guided radiofrequency ablation yields high proportions of sustained [complete responses] in properly selected patients with primary or secondary lung malignancies, and is associated with acceptable morbidity,’ write the authors.
They note that the rate of overall survival was greatly affected by the recruitment of patients with severely impaired pulmonary function, with substantial comorbidities, or both. All participants were deemed unsuitable for surgery, radiotherapy, or chemotherapy, or they had exhausted conventional treatment options. Under these circumstances, it was not possible to reliably compare radiofrequency ablation survival curves and those achieved with other treatments.
‘Additionally, the patient population was heterogeneous and included patients with NSCLC and patients with pulmonary metastases from different primary malignancies, and the study was not designed to provide evidence of survival benefits,’ they write. ‘A randomized controlled trial comparing radiofrequency ablation versus standard treatment options is now warranted to prove the clinical benefit of this approach.’”
Comment: The Lancet study findings indicate that radiofrequency ablation is a fairly safe and very effective treatment for lung metastases up to 3.5 cm in size. Importantly, the Lancet study findings indicate that there was no difference in tumor response to ablation between patients with primary lung cancer and those with secondary metastatic lung disease caused by another form of cancer originating outside of the lungs. Any women with ovarian cancer metastatic lung disease should show this study to her doctor to determine if she is eligible for radiofrequency ablation. As noted under the “Additional Studies, Clinical Trials & Other Information” section below, a 2007 U.S. study found pulmonary radiofrequency ablation for inoperable lung cancer safe and effective. Moreover, a 2006 U.S. study found radiofrequency ablation safe and effective for the treatment of ovarian cancer metastasis. Accordingly, percutaneous radiofrequency ablation can be effective in the treatment of ovarian cancer metastatic lung and liver disease for select women.
Additional Studies, Clinical Trials & Other Information:
To obtain a copy of the Phase II Clinical Trial protocol (entitled, Radiofrequency Ablation of Pulmonary Tumors Response Evaluation: a Prospective, Intention-to-Treat, Multicenter Clinical Trial) underlying the completed study above, click here.
” … ‘Despite some intriguing studies that have suggested the benefit of adjunctive antioxidant treatments in cancer patients, the totality of the available evidence is equivocal at best and leaves us with serious concerns about the potential for harm,’ Lawenda’s team concludes.”
“Cancer patients should perhaps avoid taking antioxidant supplements, a review of clinical trial data suggests, because they may diminish the effectiveness of chemotherapy and radiation treatment. Still, findings from different studies are conflicting, so further research is warranted to determine whether antioxidants can be safely taken during cancer therapy and whether they have any benefit.
In researching the impact of antioxidant use on radiation therapy, the team identified three clinical studies that specifically addressed the topic. Results from the largest of the three trials suggested that antioxidant therapy reduced overall survival. However, there was evidence indicating that one antioxidant, amifostine, can protect certain healthy tissues from radiation damage without increasing resistance in cancerous tissue. Sixteen trials were identified that looked at the effects of antioxidant supplements on chemotherapy. There was no evidence that antioxidants reduced treatment response rates, although the authors warn that none of the studies were really large enough to address this properly.
‘Despite some intriguing studies that have suggested the benefit of adjunctive antioxidant treatments in cancer patients, the totality of the available evidence is equivocal at best and leaves us with serious concerns about the potential for harm,’ Lawenda’s team concludes.”
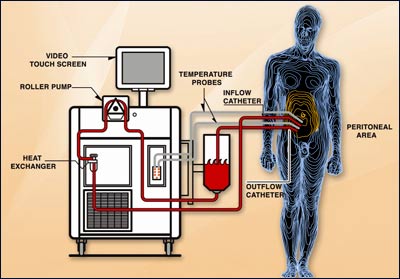
HIPEC is used in conjunction with surgery and chemotherapy to treat patients with gastrointestinal tract and gynecological cancers and sarcomas that have spread to the lining of the abdomen. Even after surgical removal, cancer often recurs in the abdomen. So when the tumor spreads, it is difficult for doctors to treat with standard chemotherapy.
HIPEC involves using a using a heated sterile solution that is circulated throughout the abdominal cavity. With HIPEC treatment, patients are connected to a series of tubes and a pumping device that bathes the abdominal cavity for two hours with a heated sterile solution containing anticancer (chemotherapeutic) drugs. The high temperature of the chemotherapy increases the effect of the drug. The fluid goes through the abdomen to treat tumor cells that may remain after surgery. Both heat and direct contact with chemotherapy drugs kills the cancer cells.
Twenty-one patients were enrolled in this Phase I clinical trial. The maximum PLD dose evaluated in this trial was 100 mg/m² and was well tolerated. The most common grade 3/4 complications were superficial wound infection and prolonged ileus. One patient developed an anastomotic leak in the postoperative period, requiring re-exploration. The length of the median postoperative hospital stay was 7 days (range, 4-29 days), three patients required readmissions within 30 days, and there were no operative deaths.
The median follow-up time for was 13.7 months (range, 3-38 months). The median overall survival was 30.6 months with a median progression free survival (PFS) of 25 months. Based on these findings, the trial investigators concluded that HIPEC with PLD following maximal cytoreduction in patients with advanced abdominal-only, gastrointestinal or gynecologic malignancies is well tolerated. Moreover, the investigators stated that the encouraging survival period after cytoreduction and HIPEC with PLD suggests that a verification Phase II clinical trial is warranted.
For more information regarding the HIPEC procedure, go to HIPECTREATMENT.org. For a list of open clinical trials testing the HIPEC procedure using various chemotherapeutic agents, click here.
The epothilones are effective antitumor medications for patients with cancer, including patients who have been previously treated with or are resistant to anthracyclines or the taxanes.
The epothilones are a novel class of antitumor medications, similar to the taxanes in some respects, but that also possess several advantages. Like taxanes, epothilones are believed to produce antitumor effects by binding to and stabilizing intracellular microtubules, which are essential in DNA replication and cell division. Several in vitro and animal studies have shown that the epothilones are more potent microtubule stabilizers than the taxanes, they are effective against cancer cell lines with high levels of drug resistance, and they induce the regression of taxane-resistant human tumors. Preclinical studies also have demonstrated synergistic increases in tumor cell killing when the epothilones are combined with other antitumor medications.
Epothilone B (patupilone/EPO906) has been evaluated in a series of phase I and II clinical trials, which demonstrated disease stabilization or objective responses in patients with a variety of cancers, including ovarian, prostate, breast, colon, stomach, and kidney cancers. This agent is currently being evaluated in phase III clinical trials. A second epothilone, ixabepilone (Ixempra™), was recently approved by the U.S. Food and Drug Administration (FDA) for the treatment of metastatic breast cancer. Ixabepilone was evaluated as a monotherapy for the treatment of breast cancer in phase II clinical trials of previously untreated patients and in taxane-experienced and taxane-resistant disease. A phase III clinical trial demonstrated that the combination of ixabepilone and capecitabine was superior to capecitabine alone in heavily pretreated, taxane-resistant patients. Ongoing clinical trials will continue to define the role of the epothilones in cancer therapy.
For a list of open clinical trials testing epothilones against ovarian cancer, click here.
On June 9, 2008, Survivorship A to Z, a new on-line resource for cancer survivors, was officially launched. The mission of Survivorship A to Z is to provide the practical information that you need to thrive in the “new normal” that exists after a life-changing cancer diagnosis. This on-line resource was founded by David S. Landay, who a graduate of the Wharton School of the University of Pennsylvania, and Harvard Law School.
Survivorship A to Z is a nonprofit corporation that provides comprehensive resources for cancer survivors including those listed below.
Get the practical information you need for all parts of your life impacted by your diagnosis in whatever depth you want – including downloadable forms.
Personalize information to your disease, stage, social and economic situation with a free, one-of-a-kind Individual Action Plan. Your plan is computer-generated. It changes as your health, economic or personal situation changes.
Start your own personal Symptoms Diary to keep track of your symptoms. With a touch of a button, you receive an instantly readable graph to show your doctor.
Use the Health Plan Evaluator to help choose the health insurance policy that is best for you considering your health condition and your particular needs. If you are Uninsured, learn how to get the care you need and how to obtain health insurance.
Use interactive charts to help maximize your financial situation. Health expenses account for over 50% of bankruptcies – including people with insurance.
Share information or concerns on the community Message Boards. Message boards are an invaluable source of shared information and support. Message boards are divided by categories such as Insurance, Finances and Employment (with separate boards for business owners, self-employed people and employees).
If you would like to watch the Good Morning America segment highlighting Survivorship A to Z that aired on June 11, 2008, click here. If you want review a list of topics covered by Survivorship A to Z, click here.
“ASCO and others in the biomedical research community are calling for Congress to increase funding for NIH by $1.9 billion (6.6%) in Fiscal Year 2009 to keep pace with medical research inflation, to reverse the effects of flat funding, and to sustain momentum in biomedical research.”
“Federal Research Funding
Increase Federal Research Funding. Make Your Voice Heard.
The fight against cancer needs your help.
Almost 1.5 million Americans will be diagnosed with cancer this year, and 1 American dies of the disease every minute.
But instead of increasing funding to find new and better cures, our nation’s commitment to funding cancer research is waning. In fact, adjusted for inflation, we have about $500 million less for cancer research than we did just five years ago.
Take Action Now. Sign ASCO’s petition to support increased funding for the National Institutes of Health and the National Cancer Institute.
Background:
The nation’s investment in cancer research is paying off. Cancer deaths are decreasing, survival rates are increasing and treatments are becoming more targeted and with fewer side-effects.
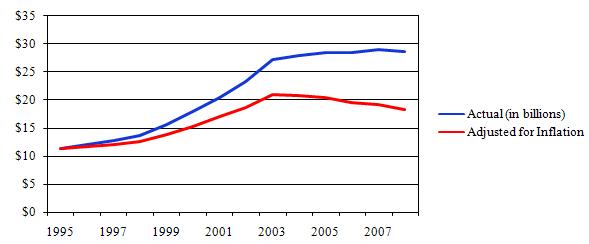
But the United States is in the midst of the longest sustained period of flat funding for cancer research. The budgets for the National Institutes of Health (NIH) and the National Cancer Institute (NCI) have been flat for 5 years. Adjusted for inflation (using the Biomedical Research and Development Price Index), the NIH budget has fallen 13 percent since 2003, and the NCI budget has fallen 12 percent since 2004.
Decline in NIH Purchasing Power: 1995-2007
(Source: Association of American Medical Colleges)
(ASCO Ad in USA Today, June 2, 2008 )
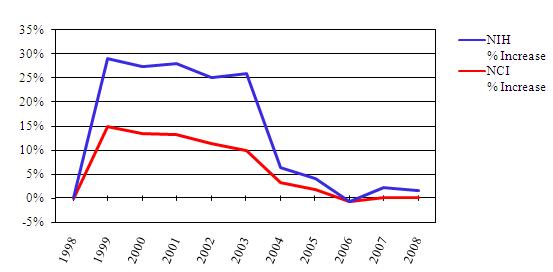
Annual Increase of NIH and NCI Appropriations 1998-2008
(Source: ASCO)
After years of progress, funding for NIH and NCI leveled off and actually decreased in recent years. From 1998 to 2003, funding for NCI increased by 80 percent, allowing for major advances in cancer research . Since that period of rapid growth, NCI’s budget has grown by an average of less than 1 percent annually. In FY 2006, NCI experienced a cut of almost 1 percent.
These declines in the value of NIH and NCI funding threaten to erode the extraordinary recent progress made in biomedical research over the past decade, at a time when scientific potential has never been greater.
ASCO Position:
ASCO and others in the biomedical research community are calling for Congress to increase funding for NIH by $1.9 billion, or 6.6 percent, in FY 2009, to keep pace with medical research inflation, to reverse the effects of flat funding and to sustain momentum in biomedical research. ASCO respects the professional judgment of the NCI in requesting a total of $5.26 billion (a $455 million increase over FY 2008 funding levels). ASCO will work to ensure that Congress approves the largest possible total funding increase to support NIH and cancer research. ASCO is also calling for funding increases over the next several years that at least keep pace with inflation to ensure that progress in cancer research continues.
“One-thousand Canadian Jewish women are being offered a chance to take a free test to find out if they are at a high risk of developing breast and ovarian cancers. Scientists with Women’s College Research Institute will screen for three inherited breast cancer gene mutations common to people of Ashkenazi Jewish ancestry with the aim of preventing the disease. …”
“One-thousand Canadian Jewish women are being offered a chance to take a free test to find out if they are at a high risk of developing breast and ovarian cancers. Scientists with Women’s College Research Institute will screen for three inherited breast cancer gene mutations common to people of Ashkenazi Jewish ancestry with the aim of preventing the disease.
Adult Jewish women in Ontario, who have no known family history of breast or ovarian cancer, are being offered a blood test to screen for three specific mutations of the BRCA1 and BRCA2 genes, beginning this Thursday in Toronto. Jewish women with a family history of breast or ovarian cancer who have never been tested are also eligible. If expanding genetic testing to this group proves worthwhile, it could change the way the testing is offered across Canada by recognizing cancer risk due to ancestry.
The goal of the test is ‘to prevent cancer,’ said Steven Narod, director of the familial breast cancer research unit at Women’s College Research Institute. He said one in 44 Ashkenazi Jewish people carry the mutation compared to the general population in which an estimated one in 400 individuals carries a mutation in BRCA1 or BRCA2. According to UIA Federations Canada, most of Canada’s Jewish population is Ashkenazi — 327,360 out of a total of 370,055 — and about half of the Ashkenazi Jewish population, 165,175 — live in Toronto.
About 70 per cent of women who are BRCA1 mutation carriers will develop breast cancer by age 70 while 40 per cent will develop ovarian cancer by the same age. Those who carry the BRCA2 genetic mutation face the same breast cancer risk as those BRCA1 mutation carriers, but their risk of developing ovarian cancer is between 15 and 20 per cent by age 70, according to Narod’s group.”
Oncolytics Biotech Inc. (“Oncolytics”) announced today that patient enrolment has started in a Phase 1/2 clinical trial for patients with metastatic ovarian, peritoneal and fallopian tube cancers using concurrent intravenous (IV) and intraperitoneal (IP)REOLYSIN®, Oncolytics’ proprietary formulation of the human reovirus. … A cell with an activated Ras Pathway, which has lost its ability to “turn off,” leads to uncontrolled cell growth. These mutations along the Ras pathway are found in approximately two-thirds of all human cancers. The virus in REOLYSIN® will invade Ras-activated cancer cells, where the virus is able to replicate until it kills the host tumor cell. When the cancer cell dies, thousands of progeny virus particles are released, which then proceed to infect and kill adjacent cancer cells.
Oncolytics Biotech Inc. (“Oncolytics”) announced today that patient enrolment has started in a Phase 1/2 clinical trial for patients with metastatic ovarian, peritoneal and fallopian tube cancers using concurrentintravenous (IV) and intraperitoneal (IP) administration of REOLYSIN®, Oncolytics’ proprietary formulation of the human reovirus. Reovirus, an acronym for Respiratory Enteric Orphan virus, is generally believed to inhabit the respiratory and bowel systems in humans. Reovirus is found naturally in sewage and water supplies. By age 12, half of all children show evidence of reovirus exposure and by adulthood, most people have been exposed. However, the disease is non-pathogenic, meaning there are typically no symptoms from infections. The link to its cancer-killing ability was established after the reovirus was discovered to reproduce well in various cancer cell lines. Reoviruses are able to replicate only in cancer cells with an activated Ras pathway, without harming healthy cells. The Ras pathway is instrumental in transferring growth signals to the nucleus of a cell, telling the cell when and how to grow-much like an “on-off” switch.
A cell with an activated Ras Pathway, which has lost its ability to “turn off,” leads to uncontrolled cell growth. These mutations along the Ras pathway are found in approximately two-thirds of all human cancers. The virus in REOLYSIN® will invade Ras-activated cancer cells, where the virus is able to replicate until it kills the host tumor cell. When the cancer cell dies, thousands of progeny virus particles are released, which then proceed to infect and kill adjacent cancer cells. The process is believed to continue until all infected cancer cells with activated Ras pathways have been infected and killed by the reovirus – all without causing the nausea, hair loss and other side effects associated with radiation and chemotherapy. More recently, Oncolytics discovered that tumor antigens generated by this virus may educate the immune system to recognize and kill tumor cells.
“REOLYSIN® is an exciting agent to investigate in patients with ovarian cancer,” said Dr. Cohn. “Targeting a specific alteration commonly present in these tumors will hopefully lead to efficacy with minimal toxicity.”
“We are looking forward to working closely with the NCI to examine the effects of using REOLYSIN® with two concurrent methods of administration,” said Dr. Brad Thompson, President and CEO of Oncolytics. “Our REOLYSIN® clinical program has now expanded to include ten Phase 1/2 or Phase 2 trials in the U.S. and the U.K. using REOLYSIN® as a monotherapy or in combination with radiation or chemotherapy.”
In the Phase 1 portion of the trial, patients will receive a constant dose of IV REOLYSIN® on days 1-5 every 28 days, as well as an escalating dose of IP REOLYSIN® on days 1-2 every 28 days. In the Phase 2 portion of the study, patients will receive a constant dose of IV REOLYSIN® on days 1-5 every 28 days as well as the Maximum Tolerated Dose (MTD) of IP REOLYSIN® from the Phase 1 portion.
The primary objectives of the Phase 1 trial are to determine the safety and tolerability of IV and IP administration of REOLYSIN®, and the MTD of IP REOLYSIN® when used with a fixed dose of IV REOLYSIN®. The primary objective of the Phase 2 trial is to determine the objective response rate of treatment with IV and IP REOLYSIN® in patients with recurrent, platinum-refractory ovarian, peritoneal and fallopian tubal carcinomas. The Phase 1/2 trial is expected to enroll up to 70 patients.
Voreloxin (at a 48 mg/m² dosage) demonstrates single agent activity in advanced platinum-resistant ovarian cancer patients (24 patients with stable disease (SD) ≥90 days, 1 patent with complete response (CR), 5 patients with partial response (PR)) as evidenced by a 48% overall disease control rate (i.e., SD + PR + CR). The results are impressive because the disease control response population includes patients with primary and secondary platinum drug resistance who have failed prior treatment with pegylated liposomal doxorubicin (Doxil®, Caelyx®, Myocet®), gemcitabine (Gemzar®), topotecan (Hycamtin®), etoposide (Eposin®,Etopophos®, Vepesid®), bevacizumab (Avastin®), and/or other various experimental agents.
The H*O*P*E*™ weblog reported the early interim success of Voreloxin (formerly known as SNS-595) in Phase II clinical trial testing on March 15, 2008. Based upon an abstract presentation that will be made by Sunesis Pharmaceuticals today at the 2008 American Society of Clinical Oncology (ASCO) Annual Meeting, the success of Voreloxin continues, despite the fact that many of the ovarian cancer patients participating in the trial experienced significant drug/treatment resistance prior to enrollment.
Specifically, Voreloxin (at a 48 mg/m² dosage) demonstrates single agent activity in advanced platinum-resistant ovarian cancer patients (24 patients with stable disease (SD) ≥90 days, 1 patent with complete response (CR), 5 patients with partial response (PR)) as evidenced by a 48% overall disease control rate (i.e., SD + PR + CR). The results are impressive because the disease control response population includes patients with primary and secondary platinum drug resistance who have failed prior treatment with pegylated liposomal doxorubicin (Doxil®, Caelyx®, Myocet®), gemcitabine (Gemzar®), topotecan (Hycamtin®), etoposide (Eposin®, Etopophos®, Vepesid®), bevacizumab (Avastin®), and/or other various experimental agents. Approximately 79% of the patient population that experienced disease control with Voreloxin at a 48mg/m² dosage received between two to four prior lines of treatment. In addition, one patient who experienced a partial response to Voreloxin at the 48 mg/m² dosage had a tumor histology identified as clear cell ovarian cancer — an aggressive form of ovarian cancer that is generally resistant to traditional therapies. It appears that there are 11 clear cell ovarian cancer patients participating in the Voreloxin Phase II trial (i.e., 7 patients in the 48 mg/m² dosage arm, and 4 patients in the 60 mg/m² dosage arm); however, there are no specific results reported for these patients (other than the one partial responder) in the 2008 ASCO Annual Meeting abstract presentation data.
Due to the earlier success of Voreloxin prior to March 15th, the trial investigators enrolled 21 new patients into the Phase II trial for purposes of testing Voreloxin at a 60 mg/m² dosage. Because these newer patients only received two cycles of Voreloxin at the higher dosage to date, they were not evaluated officially for purposes of the 2008 ASCO Annual Meeting abstract presentation data. The grade 3/4 adverse effects of Voreloxin at both dosages are reported as relatively low, therefore, trial investigators incorporated a 75 mg/m² dosage escalation into the current Phase II trial. The investigators do not indicate how many patients (currently enrolled or newly recruited) will participate in the 75 mg/m² dosage arm. Currently, a total of 86 ovarian cancer patients are enrolled in the Voreloxin Phase II trial (65 patients in the 48 mg/m² dosage arm; 21 patients in the 60 mg/m² dosage arm).
“Stand Up To Cancer (www.standup2cancer.org), a new initiative to raise philanthropic dollars for accelerating ground-breaking research, launches today through an unprecedented collaboration uniting the major television networks, entertainment industry executives, celebrities and prominent leaders in cancer research and patient advocacy. ABC, CBS and NBC will donate one hour of simultaneous commercial-free primetime for a nationally televised fundraising event to air on September 5, 2008 (8:00 pm EDT and PDT), aimed at rallying the public around the goal of ending cancer’s reign as a leading cause of death. … Stand Up To Cancer’s innovative approach to research is designed to eliminate barriers that have traditionally inhibited creativity and collaboration by enabling the best and brightest investigators from leading institutions across the country and internationally to work together. These collaborative “Dream Teams” will pursue the most promising research, accelerating the discovery of new therapies for cancer patients and advancing efforts in cancer prevention research.Stand Up To Cancer monies will also be used for some high-risk, high-impact cancer research proposals, which are often not supported by conventional funding sources.”
“Stand Up To Cancer (www.standup2cancer.org), a new initiative to raise philanthropic dollars for accelerating ground-breaking research, launches today through an unprecedented collaboration uniting the major television networks, entertainment industry executives, celebrities and prominent leaders in cancer research and patient advocacy. ABC, CBS and NBC will donate one hour of simultaneous commercial-free primetime for a nationally televised fundraising event to air on September 5, 2008 (8:00 pm EDT and PDT), aimed at rallying the public around the goal of ending cancer’s reign as a leading cause of death.
‘For people struggling with this disease, or those who will be diagnosed, scientific breakthroughs can be a matter of life or death — literally. We want everyone to know that they can make a difference in this fight,’ said Couric. ‘Television is a notoriously competitive business. For the three major broadcast networks to join forces is a wonderful example of the power of working together, and we’re very grateful to have the opportunity to reach people all over the country through this show.’
‘As a motion picture and television producer, I’ve learned how incredibly powerful these mediums can be in generating public discourse, sometimes almost overnight. Our goal with this initiative and TV show is to ‘tip’ the conversation in this country about cancer – to get people riled up, so they want to do something about the fact that it still takes so many lives,’ said Laura Ziskin, who will produce the September 5th broadcast. Ziskin is a cancer survivor. Her film credits include the Spider-Man trilogy, As Good As It Gets, and Pretty Woman, and she also produced the 74th and 79th Annual Academy Awards.
The Stand Up To Cancer special will feature live performances by legendary recording artists and stars from film and television who will perform as well as present filmed content giving viewers insight into cancer. Various screening tests will be demonstrated in novel and entertaining ways. ‘Katie, Charlie and Brian will report on potentially life-saving research, speaking with both patients and scientists. We hope to entertain you, educate you, move and inspire you,’ Ziskin said.
Stand Up To Cancer (SU2C) is a program of the Entertainment Industry Foundation (EIF), a 501(c)(3) charitable organization, and was established by a group of media, entertainment and philanthropic leaders, whose lives have all been affected by cancer in significant ways. Stand Up To Cancer is bringing industry resources — people, as well as mediums such as television and the web — to bear in the fight against cancer as never before.
‘The statistics are staggering,’ Gibson said. ‘Cancer claims one person every minute of every day in the United States. Every year in this country, it takes the lives of more than half a million people…worldwide, cancer kills more than six million people annually. There has been progress on both the research and awareness fronts; as a result, there are over ten million cancer survivors in the US today. More work urgently needs to be done so that more people will survive,’ he said.
‘Not only has cancer touched all of our media organizations in profound ways, but it has touched each of us personally. This extraordinary broadcast will serve a number of purposes – we’ll share vital information with our viewers and hopefully raise funds that are so critical in the fight against this insidious disease,’ said Williams.
New developments in the laboratory are revealing the way cancer begins, progresses and spreads. Stand Up To Cancer is founded on the belief that now, more than ever, there is sufficient knowledge of the basic science of cancer, and that the technologies are finally available to translate this knowledge into real advances in treatment and prevention. Today’s cancer scientists are on the verge of life-saving discoveries. But what they desperately need are the funds required to mount an all-out assault. Stand Up To Cancer is dedicated to providing this much needed new source of cancer research funding.
Co-Chair of the Disney Media Networks and President of the Disney-ABC Television Group Anne Sweeney, CBS Corporation President and Chief Executive Officer Leslie Moonves, and NBC Universal President and Chief Executive Officer Jeff Zucker commented on their companies’ decisions to collaborate.
‘Everyone in our country has been touched by cancer in some way, shape or form. The thought that we could, in one hour of television, make a true difference in the fight against this disease was both exciting and inspiring,’ Sweeney said.
‘Television is a uniquely powerful medium and the networks joining forces offer an unparalleled opportunity to communicate loud and clear that we all have a stake in the fight against cancer,’ said Moonves. ‘Through the unity of broadcasters, entertainers and cancer groups alike, and the giving spirit of the audience at home, this television event has the potential to make a profound impact on our society’s ability to understand and battle this terrible disease.’
‘We’ve gone to the moon and pioneered a technology that revolutionized the way the world communicates. Applying that same innovation and commitment, scientists are on the cusp of making enormous strides in their efforts to combat cancer, but they need additional funding to do that. Through Stand Up To Cancer, and the September 5th broadcast, people all over the country can help,’ said Zucker, who is a cancer survivor.
AN INNOVATIVE RESEARCH MODEL
Stand Up To Cancer’s innovative approach to research is designed to eliminate barriers that have traditionally inhibited creativity and collaboration by enabling the best and brightest investigators from leading institutions across the country and internationally to work together. These collaborative “Dream Teams” will pursue the most promising research, accelerating the discovery of new therapies for cancer patients and advancing efforts in cancer prevention research. Stand Up To Cancer monies will also be used for some high-risk, high-impact cancer research proposals, which are often not supported by conventional funding sources.
The American Association for Cancer Research (AACR) will conduct expert scientific review of the research projects and administer funds raised through the initiative under the direction of a Scientific Advisory Committee. Nobel Laureate Phillip A. Sharp, Ph.D., Institute Professor at the Massachusetts Institute of Technology and the David H. Koch Institute for Integrative Cancer Research at MIT chairs the Committee, which includes highly accomplished clinical investigators, senior laboratory researchers and physician-scientists. ‘This project has tremendous potential to change the face of cancer research,’ said Sharp. ‘Our goal is to rapidly move new research discoveries out of the lab and into the clinic to save lives from cancer.’
‘I am pleased that AACR is a partner in the Stand Up To Cancer initiative,’ said Raymond N. DuBois, M.D., Ph.D., AACR President and Provost and Executive Vice President at M. D. Anderson Cancer Center. ‘Stand Up To Cancer model is distinctive because it emphasizes collaboration among scientists and will accelerate translational research on the verge of breakthroughs as well as provide an additional revenue stream to encourage novel, high-risk proposals that have great potential in making inroads against cancer.’
A Stand Up To Cancer Advocate Advisory Council is being formed, and will include leaders from approximately 25 organizations. Additionally, representatives from the advocacy community will work side-by-side with the scientists on the “Dream Teams,” so the perspectives of the patients and survivors they represent will be integrated into the direction of the research.
INITIATIVE DETAILS
In addition to the nationally televised network fundraising event, other key elements of the initiative include:
• Standup2cancer — With both interactive applications and rich content, the SU2C web site will foster an online community for everyone affected by cancer, utilizing the same approach as the televised special: it will move, educate and even entertain users. Features include: The Constellation: For a dollar donation or more, users can launch a star in honor of anyone who has received a cancer diagnosis. The Stand: An interactive facebook application to illustrate that the ‘cancer community’ encompasses everyone and that we are all connected by this disease. SUTV: Features video segments rich in scientific and research information, as well as ones that confront the personal and human side of cancer’s impact. SU2C Magazine: Offers seven sections of diverse content written by leading voices in every field.
• Public Service Announcement (PSA) Campaign – A series of TV, radio and print PSAs featuring celebrities and members of the general public to mobilize support for the campaign will begin to air and appear in publications soon.
‘I have lost beloved family members and friends to this dreaded disease,’ said Sherry Lansing. ‘Sometimes I feel as if cancer is an epidemic that will never end. But then I am reminded of diseases such as tuberculosis, small pox and polio that used to cause fear… and then I know that just like those other diseases, cancer can and will be defeated, too.’
Major League Baseball was the first donor to contribute to Stand Up To Cancer. ‘This initiative has presented an historic and unique plan to fight this deadly disease, and it is a privilege for me and Major League Baseball to join this magnificent effort,’ said Baseball Commissioner Allan H. (Bud) Selig. ‘We have pledged many of our valuable resources in an attempt to assist in every way we can.’
The American Association for Cancer Research (AACR) is the oldest and largest scientific organization in the world focusing on every aspect of high-quality, innovative cancer research. Its reputation for scientific breadth and excellence attracts the premier researchers in the field. By accelerating the growth and spread of new knowledge about cancer, the AACR is on the front lines in the quest for the prevention and cure of cancer.
About the Entertainment Industry Foundation
The Entertainment Industry Foundation (EIF), as a leading charitable organization of the entertainment industry, has distributed hundreds of millions of dollars to support programs addressing critical health, education and social issues.
About the Noreen Fraser Foundation
The Noreen Fraser Foundation utilizes film, television and web technologies to raise money as well as to educate and raise awareness about women’s cancers. The funds raised will be used to provide large grants to uniquely qualified cancer researchers.
# # #
Media Contacts:
Ketchum Global Media Network Nicholas Scibetta — 646.935.4067 or 917.873.5299 mobile nicholas.scibetta@ketchum.com
Comment: In 1971, President Nixon “declared war on cancer.” Unfortunately, the technology and science of the 1970’s was simply not advanced enough to accomplish such a goal. The complexities of cancer are many including the following: (i) the area of “cancer” encompasses approximately 200 separate diseases, and (ii) the biological processes that allow cancer to thrive are nearly identical to those that allow a single cell, fertilized embryo to grow into a one trillion cell adult human. If you fast forward to this past decade, it is clear that current day technology and science is capable of achieving the short-term goal of holding cancer in check while pursuing the long-term goal of a cure. Discovery and identification of the human genome (Adobe Reader PDF document) in tandem with the mapping of biological “cellular pathways,” have produced highly successful advanced targeted cancer therapies such as Gleevec® and Herceptin®. The Human Genome Project identified approximately 20,500 genes in the human DNA sequence, and to date, that project fueled – in large part – the discovery of approximately 1,800 “disease genes” (Adobe Reader PDF Document). Our current ability to identify numerous genetic anomalies in cancer cells quickly, simultaneously and cost effectively allows for the targeting of such anomalies through pharmacological drug and/or gene therapy. Super computers allow scientist to generate the extensive bioinformatics necessary to produce complex models and analyze study data involving millions of permutations associated with 20,500 human genes, which hold approximately 3 billion pieces of DNA information. Although in its infancy, the use of “silencing RNA” (siRNA) to turn various genes on or off is making great strides toward controlling cancer in vitro and in vivo.
Human epigentics – another missing piece to the cancer puzzle – is the subject of the Human Epigenome Project, which is being conducted by the Human Epigenome Consortium. The Human Genome Project provided the blueprint for life, but the Human Epigenome Project will tell us how the human genome gets executed, as well as what determines when and where genes are switched on and off. The best example of epigenetics at work is the case of identical twins, where one twin is autistic while the other twin is normal. In this case, the genome DNA sequence of both twins is identical, but something else causes a change. That “something else” is represented by chemical modifications of genes that act as green or red traffic lights, which are superimposed on top of the DNA sequence or genome and tell the genes whether to be active or inactive. The study of these modifications-what they are, how they are laid down, and the processes that they control-is the field of research known as “epigenetics.” An “epigenome” is the description of these chemical modifications across the whole genome, but unlike the genome DNA sequence, each organism has multiple epigenomes-for example, in different cell types-that may change during its lifetime in response to environmental conditions or cues. And, knowing more about the human epigenome may provide clues as to what goes wrong in cancer and other diseases. Human Epigenome Project-Up and Running, Bradbury J.; PLoS Biol 1(3): e82 (2003).
The Stand Up to Cancer paradigm is truly groundbreaking.It is designed to “end run” bureaucratic obstacles to cancer control and cure discoveries. Through world-class private sector philanthropy, the medical, biological, genetic, and translational research necessary to tackle this ambitious goal will be carried out in a fully coordinated effort by the brightest scientific minds in the nation and around the world. Under the Stand Up To Cancer approach there will be accountability for results and oversight to guard against conflicts of interest. If you carefully review the names of those directly or indirectly associated with the Stand Up to Cancer organization, you will discover that they represent those individuals, scientists, and companies that had the greatest impact – through fundraising or science – on cancer therapy developments and discoveries over the past decade. I provide below the Stand Up To Cancer Public Service Announcement video, along with an additional video featuring the Stand Up To Cancer news coverage by CBS. To view additional Stand Up To Cancer videos featuring Katie Couric, Larry David, Sidney Poitier, Robert Bazell, Ben Teller & other celebrities who support the movement, click here.
What Can You Do?: Stand Up To Cancer invites donations in many forms. For a contribution of $1.00 or more, you can “create a star” as part of the Constellation program in the name of a cancer survivor or in memory of a family member or friend who lost the battle to cancer. On a larger scale, you can form a “private” team and request donations from family, friends, and co-workers. Alternatively, if you do not want to form a private team, consider making a donation to the “Choose H*O*P*E*” open team that was formed recently by the H*O*P*E*™ weblog or make a standalone donation. In the future, you will even be able to donate through your cell phone. Through any form of donation, you are making a difference in the fight against cancer!
“When someone is going through a life-threatening illness, one of the greatest gifts to receive is the out-pouring love and support from the community,” Totushek said. “I have no idea how many people helped me, but I know I couldn’t have done it without them. You don’t have to know someone to help them.” Mitchell is grateful to Totushek and the girls for putting on the clinic. “I’m very surprised and humbled,” Mitchell said. “It’s a strange feeling that someone I never meant would want to do something so generous. She’s a hero.”
“Maria Totushek is all too familiar with cancer.
Though now in remission from breast cancer, which was diagnosed four years ago, Totushek remembers everything about the disease, including the love and support she received from family, friends and even from people she didn’t even know.
Now Totushek, along with a big assist from some Folsom teens, is helping someone else battling cancer. This isn’t a family member or friend. In fact, it’s someone none of them have never ever met.
Kindra Mitchell, 45, lives in Reno, NV, with her husband, Jerry, and is currently battling ovarian cancer. Mitchell, a mother of three girls ages 15 to 23, is friends with Jeff Phillips, a teacher at Blanche Sprentz Elementary School in Folsom [California], who also is a good friend of Totushek and lent a big hand to her when she was battling cancer. When Phillips told Totushek about his ailing friend, Totushek had to do something.
‘When someone is going through a life-threatening illness, one of the greatest gifts to receive is the out-pouring love and support from the community,’ Totushek said. ‘I have no idea how many people helped me, but I know I couldn’t have done it without them. You don’t have to know someone to help them.’ Mitchell is grateful to Totushek and the girls for putting on the clinic. ‘I’m very surprised and humbled,’ Mitchell said. ‘It’s a strange feeling that someone I never meant would want to do something so generous. She’s a hero.’
Totushek, who has four soccer-playing daughters between the ages of 12 and five, came up with the idea to hold a soccer clinic with all the proceeds going to Mitchell. The clinic, to be held next month, is called the Kick it for Kindra Soccer Clinic and Fundraiser. Since coming up with the idea, Totushek has left a majority of the details to some Folsom teens. To Totushek, this is where the true story lies. ‘These soccer-loving teens are coming together to support a family battling ovarian cancer,’ Totushek said. ‘The girls have taken on the goal to help raise money for a family in need. They’re volunteering their time and talent to give back to the community. I hope other teens can be inspired and people in the community can see that to help someone in need can turn into a blessing for an entire community.’
The teens working on the project include Vista del Lago freshmen Alexis Reinbolt and Catherine Lehman, Folsom High sophomore Laura Cox and freshman Chelsea Cino and St. Francis freshman Beth Balbierz. The girls have been meeting over the last month, planning the drills and skills to be taught at the clinic. All are enthusiastic about the clinic. ‘It’s a blessing to me because I love soccer and I’m helping someone out at the same time,’ Reinbolt said. ‘I’ve learned a lot about myself since I became involved in it.’ For Cox, cancer is something that she’s dealt with personally. ‘My grandma is a breast cancer survivor and I’m very grateful for that,’ Cox said. ‘My grandfather died of lung cancer. I know how families struggle with cancer. I really wanted to do something to fight against it.’ Like Reinbolt, Cino and Balbierz said they wanted to help with the clinic because of their love for soccer and because it’s for a good cause. As for Lehman, it’s an opportunity to help someone in need. ‘If I was in her position, I’d want someone to help me,’ Lehman said. ‘It feels good to give back, because a lot of people don’t get that opportunity. I never thought to do something like this, but I’m having a lot of fun with it. It feels good to be able to help someone.’
Totushek’s oldest daughter, 12-year-old Madison, has also chipped in and helped her mom with a lot of the behind-the-scenes work encompassing little yet often overlooked details.
There are three sessions to the Kick it for Kindra Soccer Clinic and Fundraiser. The clinic is for boys and girls ages five to nine years old and will be held June 7-8 from 10 to 11:30 a.m., June 10 and 12 from 6 to 7:30 p.m. and on June 21-22 from 10 to 11:30 a.m. The camp will be held at Ed Mitchell Park and costs $35. All the proceeds of the clinic will go the Mitchell family. ‘Right now we’ve got 50 kids signed up,’ Totushek said. ‘We can accommodate 300, but I’d be thrilled if we got 100.’
Anyone interested in participating in the camp can e-mail Totushek at mariatotushek@folsomsoccerclub.org or visit www.folsomsoccerclub.org for more details.”
[Title Quote: The expression “pay it forward” is used to describe the concept of third party beneficiary in which a creditor offers the debtor the option of “paying” the debt forward by lending it to a third person instead of paying it back. In 2000, Catherine Ryan Hyde’s novel Pay It Forward was published and adapted into a Warner Brothers film bearing the same title. In Hyde’s book and the movie, “paying it forward” is described as an obligation to do three good deeds for others in repayment of a single good deed that one receives. Such good deeds should be things that the other person cannot accomplish on his or her own. In this way, the need to help one another can spread exponentially through society, creating a social movement with the goal of making the world a better place. The idea of the book has been championed in real life by the Pay It Forward Foundation. The Foundation focuses on bringing the idea of paying it forward to school age children, parents, and educators. The simple idea of doing good works for others to repay the good works received is easily conveyed to children and encourages them to be socially aware and take a role in making the world a better place. The main character of the book was a 12-year-old child, thus giving other children a similarly young role model to emulate.]
“Kellogg, an associate professor of pathology and laboratory medicine at the Brody School of Medicine at [East Carolina University] ECU, created the antibody, called DS-6, that attaches to cancer cells in her laboratory at ECU. DS-6 will serve as a delivery vehicle for a highly potent cell-killing agent developed by ImmunoGen specifically for delivery to cancer cells by antibodies. The antibody latches on to tumor cells and enables the whole compound – the antibody and the attached cell-killing agent – to enter the cancer cell. Once inside, the cell-killing agent becomes activated and kills the tumor cell as it divides.”
“A discovery by an East Carolina University pathologist might be a breakthrough in an evolving class of drugs used to fight cancer.
Dr. Anne Kellogg has developed a monoclonal antibody that could play a vital role in treating the most common form of ovarian cancer, breast cancer and other cancers. She is working with two major drug firms, ImmunoGen Inc. and sanofi-aventis, that have expertise in formulating antibodies into cancer therapies and taking them to clinical trials in humans.
Kellogg, an associate professor of pathology and laboratory medicine at the Brody School of Medicine at ECU, created the antibody, called DS-6, that attaches to cancer cells in her laboratory at ECU. DS-6 will serve as a delivery vehicle for a highly potent cell-killing agent developed by ImmunoGen specifically for delivery to cancer cells by antibodies. The antibody latches on to tumor cells and enables the whole compound – the antibody and the attached cell-killing agent – to enter the cancer cell. Once inside, the cell-killing agent becomes activated and kills the tumor cell as it divides.
‘We can’t give such a potent chemotherapy agent on its own because it would be too toxic, but if we can link it to an antibody, it goes inside the tumor cell and is released inside the tumor cell, which is really an amazing feat,’ Kellogg said.
The antibody with the cell-killing agent linked to it circulates in the body in an inactive state. The cell-killing agent becomes active only when it reaches the tumor cell, so ImmunoGen refers to its technology as Tumor-Activated Prodrug, or TAP, technology. Sanofi-aventis has rights to develop specific anticancer agents using ImmunoGen’s TAP technology and is in charge of advancing the TAP compound containing the DS-6 antibody licensed from ECU into human clinical testing.
Monoclonal antibodies are manufactured proteins, produced from a single parent cell, that bind to a specific substance. They can be used to detect or purify that substance and are widely used in hospital and pathology laboratories as components of diagnostic tests. Monoclonal antibodies gained attention as a possible way to treat cancer in the 1980s. In the 1990s, scientists refined techniques to expand their usefulness as therapeutics by making subtle changes to the antibodies so the human body would not reject them as foreign tissue. One of the best-known monoclonal antibodies is trastuzumab, sold under the brand name Herceptin and used to treat breast cancer.
Kellogg began working with monoclonal antibodies in the early 1990s looking for ones pathologists could use to diagnose cancer. A few years later, working with Dr. Diane Semer, a gynecologic oncologist formerly with ECU, Kellogg turned her attention to identifying an antibody that could not only recognize tumors but also be useful in treating them. She isolated DS-6 in the late 1990s and then began characterizing the antibody for its ability to recognize various types of cancer with the help of Dr. Nancy Smith, a former ECU pathologist.
‘Drugs that are developed from monoclonal antibodies are potentially more specific for tumors and risk less in the way of toxicity to the patient,’ said Dr. Adam Asch, associate director of the Leo W. Jenkins Cancer Center at ECU. Kellogg added that the treatment could have benefits even if it falls short of curing cancer. ‘You may be able to convert cancer to a very chronic disease you can treat if we can provide oncologists with a wider array of treatment options,’ she said.
‘This has been an amazing education for me and personally very rewarding to get a ringside seat in seeing the complex process of drug discovery and development take place. It has also demonstrated how well academia, biotechnology and pharmaceutical companies can work together in this process,’ Kellogg said.
Kellogg’s research has been funded in part by ECU and the Department of Pathology and Laboratory Medicine. ‘We feel we made a wise investment that will help advance the treatment of cancer by providing funds for Dr. Kellogg’s research,’ said Dr. Peter Kragel, chair of the department. Future grants from ImmunoGen and sanofi-aventis are under discussion.”
“By inhibiting MMP-2 [matrix metalloproteinase-2] activity early in the disease course, Lengyel and colleagues were able to prevent injected ovarian cancer cells from attaching to their target tissues in the peritoneum and omentum. This reduced the growth of new tumors by 68 percent, when measured four weeks after treatment. The inhibitor nearly doubled survival time in mice that were injected with ovarian cancer cells. Those who received it survived an average of 63 days, compared to untreated mice, who survived only 36 days. Brief and early intraperitoneal treatment with an MMP inhibitor, the authors conclude, may reduce peritoneal attachment, reduce metastases and significantly prolong survival.”
“A drug that blocks production of an enzyme that enables ovarian cancer to gain a foothold in a new site can slow the spread of the disease and prolong survival in mice, according to a study by researchers from the University of Chicago Medical Center, but only if the drug is given early in the disease process.
In the April issue of the Journal of Clinical Investigation, the researchers show that an enzyme known as MMP-2 is necessary for ovarian cancer to attach itself to the sites where it tends to spread. Several drugs known as MMP inhibitors (for example, marimastat or prinomastat) inhibit the enzyme, dramatically reducing the tumor’s ability to establish itself at sites beyond the ovary. But such MMP inhibitors, which were abandoned after they failed to extend survival in earlier clinical trials, have to be given before the cancer has spread.
‘Our study suggests that MMP-2 inhibitors could have a significant impact on ovarian cancer but only if administered quite early, before the cancer has advanced beyond the ovary,’ said Ernst Lengyel, assistant professor of obstetrics and gynecology at the University of Chicago.
This approach could help women who receive surgical treatment while the disease is still limited to the ovary as well as those who have successful surgery to remove all evidence of local spread of the disease. In the earlier trial, marimastat was given to women with late-stage disease that had already spread.
The fifth leading cause of cancer death in women, ovarian cancer — unlike breast, colon or lung cancer — tends to spread within the abdominal cavity and not to distant organs. Carried by fluid, it most often spreads throughout the peritoneal cavity and to the omentum, a large fat pad draped over the small bowel.
Lengyel and colleagues wanted to understand the many steps required for ovarian cancer to dislodge from its original site and establish itself elsewhere in the peritoneal cavity. They found that one of the key steps was production of MMP-2 by cancer cells that came in contact with the cells that line the peritoneal cavity.
When ovarian cancer cells make contact with the cells that line this internal cavity, they produce MMP-2 (an acronym for matrix metalloproteinase-2). MMP-2 alters two proteins–vitronectin and fibronectin–found on the surface of the cells that line the cavity. These alterations change those proteins in a way that enables the cancer cells to latch on to them better. Once attached, the cancer cells can multiply rapidly and invade.
By inhibiting MMP-2 activity early in the disease course, Lengyel and colleagues were able to prevent injected ovarian cancer cells from attaching to their target tissues in the peritoneum and omentum. This reduced the growth of new tumors by 68 percent, when measured four weeks after treatment.
The inhibitor nearly doubled survival time in mice that were injected with ovarian cancer cells. Those who received it survived an average of 63 days, compared to untreated mice, who survived only 36 days.
Brief and early intraperitoneal treatment with an MMP inhibitor, the authors conclude, may reduce peritoneal attachment, reduce metastases and significantly prolong survival.
The treatment has much less impact, however, once cancerous cells have attached and formed colonies. In several earlier trials, marimastat, an oral MMP inhibitor, was given for a prolonged period of time to women with late-stage disease that had already spread.
‘MMP-inhibitors were given at the wrong time for too long, causing side effects,’ Lengyel said. Attachment is the first step for metastatic spread. MMP-2, the target of MMP inhibitors, plays a role in early cancer spread.
‘Our study examines the initial step of ovarian cancer metastasis,’ the authors note, when cancer cells meet unprepared target cells. Other steps in this process, they suggest, may also provide additional treatment targets.
Comment: The in vivo study discussed above suggests that the use of MMP inhibitors, e.g., marimastat or prinomastat, to treat an early stage ovarian cancer patient may prevent the spread of ovarian cancer outside of the peritoneal cavity.
“We found that patients who received topotecan plus thalidomide showed an overall response rate of 47 percent compared to 21 percent response in patients who received only topotecan”‘ [Levi]Downs[Jr., M.D.] said. “In patients receiving topotecan plus thalidomide, 30 percent achieved a complete response, meaning the cancer went away, compared to 18 percent for patients only getting topotecan.” “Furthermore, patients getting topotecan plus thalidomide had a longer cancer-free period after treatment than those receiving topotecan alone,” he said.
“Thalidomide, a drug blamed in the 1950s for causing birth defects, is now showing promise as a safe and effective treatment for women with recurrent ovarian cancer, according to a study led by a University of Minnesota Cancer Center researcher.
‘For some women, ovarian cancer has become a chronic disease,’ Downs said. ‘The standard chemotherapy regimens can put recurrent cancer in remission, often more than once. However, when the cancer resists the standard treatments, we need new options for treatment.’
The study compared the effectiveness and safety of the combination of thalidomide and topotecan, a chemotherapy often used for ovarian cancer, versus topotecan alone for treatment of recurrent epithelial ovarian cancer in patients who had received prior treatment. Epithelial ovarian cancer is a disease in which cancer cells form in the tissue that covers the ovary.
The study evaluated 75 women who were randomly assigned to receive either the combination of thalidomide and topotecan or only topotecan. This is the first randomized clinical trial to test thalidomide for recurrent ovarian cancer. Other clinical trials have shown thalidomide to be effective for treatment of multiple myeloma, a cancer of the bone marrow.
‘We found that patients who received topotecan plus thalidomide showed an overall response rate of 47 percent compared to 21 percent response in patients who received only topotecan,’ Downs said. ‘In patients receiving topotecan plus thalidomide, 30 percent achieved a complete response, meaning the cancer went away, compared to 18 percent for patients only getting topotecan.’
‘Furthermore, patients getting topotecan plus thalidomide had a longer cancer-free period after treatment than those receiving topotecan alone,’ he said. ‘What all of this means is that while thalidomide may not cure ovarian cancer, it may broaden the treatment options available to physicians and provide more hope to women diagnosed with the cancer.’
Ovarian cancer is the fifth most common cancer among women. This year in the United States, more than 25,000 women will be diagnosed with ovarian cancer, and about 16,000 will die from it. About 78 percent of women diagnosed with the cancer survive one year after diagnosis, and more than 50 percent survive five years after diagnosis.
The results of this study have led to the development of a new clinical trial at the University of Minnesota that will test the safety and effectiveness of a newer member of the class of drugs containing thalidomide properties for treatment of recurrent ovarian cancer.
This study was sponsored by Celgene Corporation, biopharmaceutical company and manufacturer of thalidomide. Cancer centers in Minnesota, Ohio, South Dakota, and California participated in this study.